ARFID is a feeding and eating disorder where a teen avoids or restricts food so severely that their health, growth, or daily life suffers. The eating is not driven by worries about weight or body shape, which sets it apart from other eating disorders.
Many parents first notice a teen who eats only a short list of safe foods, panics at new textures, or seems to have almost no appetite. These patterns can look like extreme picky eating, yet they run deeper and last far longer.
Avoidant restrictive food intake disorder (ARFID) became an official diagnosis in 2013 and affects teens of every body size. Knowing what it is, why it happens, and how it responds to care helps families act early.
Key Takeaways
- The American Psychiatric Association classifies avoidant restrictive food intake disorder in the DSM-5-TR, and the World Health Organization lists it under ICD-10 code F50.82 and within ICD-11.
- A 2022 Harvard study reported that more than half of people with ARFID also live with another neurodevelopmental, psychiatric, or medical condition, with anxiety the most common companion.
- Research reviews estimate that between 8% and 55% of children diagnosed with ARFID are also autistic, largely because both involve heightened sensory sensitivity.
- Clinicians sort ARFID into sensory-based avoidance, low interest in eating, and fear of aversive consequences such as choking or vomiting.
- Structured therapies such as CBT-AR and family-based treatment widen a teen's food range before nutritional deficiency or faltering growth takes hold.
What Is ARFID?
ARFID (Avoidant/Restrictive Food Intake Disorder) names a feeding and eating disorder in which a teen limits the amount or variety of food they eat, producing weight loss, nutritional deficiency, supplement dependence, or marked disruption to daily functioning. Unlike anorexia nervosa, ARFID does not stem from body image disturbance or a fear of weight gain.
The DSM-5-TR groups ARFID alongside pica and rumination disorder under feeding and eating disorders. It affects teens at high, average, and low weights, so a normal-weight adolescent can still meet full diagnostic criteria.
When Does ARFID Develop?
ARFID typically begins in early childhood and intensifies across adolescence as growth demands outpace a shrinking diet. The following stages show how the disorder commonly unfolds when it goes unaddressed.
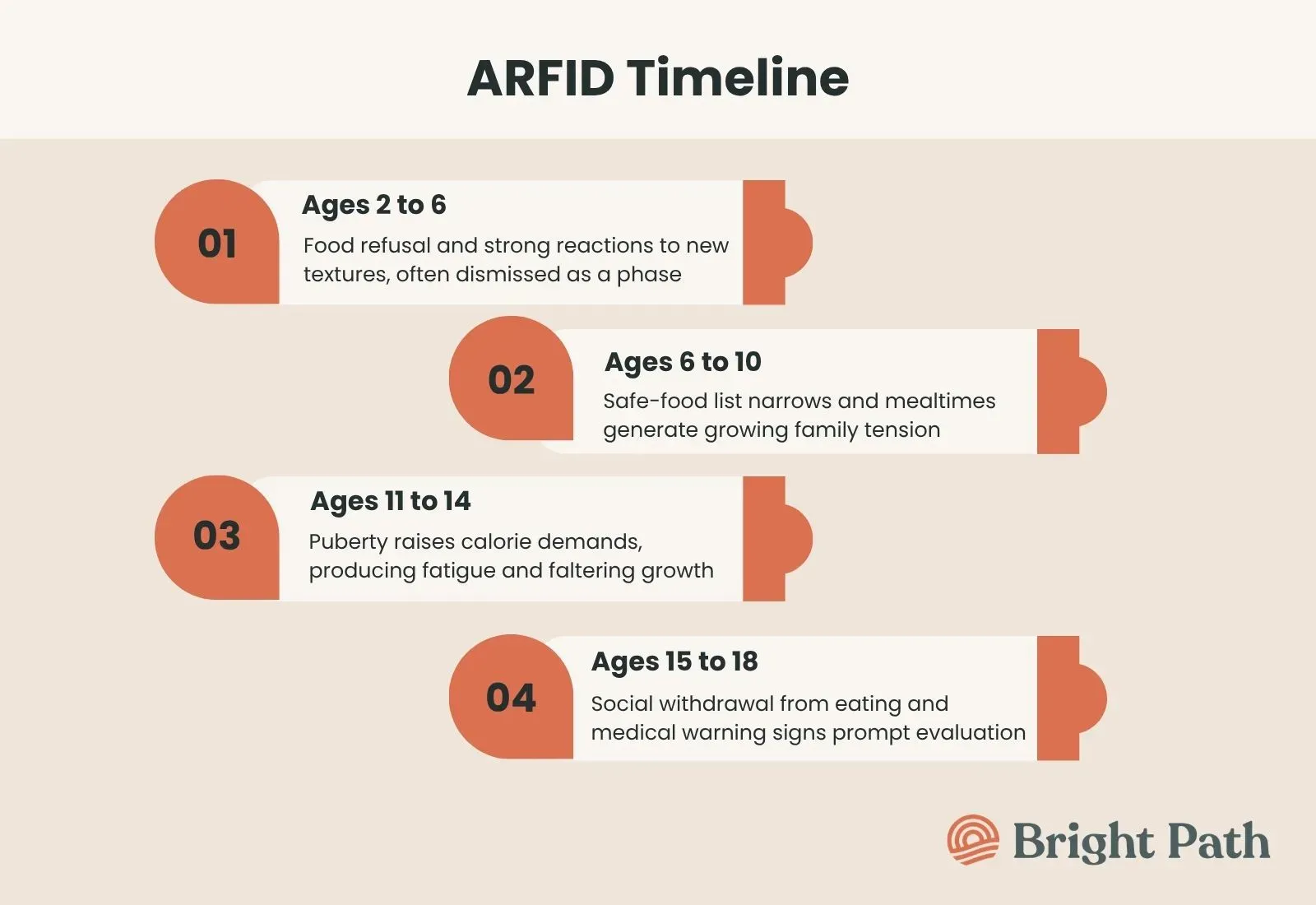
- Ages 2 to 6: Food refusal and strong reactions to new textures appear, often dismissed as a passing toddler phase.
- Ages 6 to 10: The safe-food list narrows, and mealtimes generate growing tension between the child and caregivers.
- Ages 11 to 14: Puberty raises calorie and nutrient demands, so a limited diet starts producing fatigue, micronutrient deficiency, and faltering growth.
- Ages 15 to 18: Social withdrawal from eating, mealtime anxiety, and medical warning signs such as dizziness or delayed puberty often surface and prompt evaluation.
What are the Subtypes of ARFID?
ARFID divides into three recognized subtypes, and each subtype channels food avoidance through a different underlying driver. A teen can show one pattern or a blend of all three.
- Sensory-based avoidance: Sensory-based avoidance drives a teen to reject foods because their texture, smell, color, or taste overwhelms the senses. This subtype shows the strongest link to autism spectrum disorder and to sensory processing differences.
- Low interest in eating: Low interest in eating leaves a teen with little appetite and faint hunger signals, so meals feel like a chore rather than a need. This subtype reflects weak interoceptive awareness, meaning the brain registers hunger poorly.
- Fear of aversive consequences: Fear of aversive consequences pushes a teen to avoid eating after a frightening event such as choking, vomiting, or severe stomach pain. This subtype frequently connects to emetophobia, the intense fear of vomiting, and to specific phobia.
What Are the Symptoms of ARFID?
ARFID symptoms span behavior, physical health, and social life, and they intensify as restriction continues. The signs sort into everyday patterns, urgent medical red flags, and long-term consequences.
Common Signs of ARFID
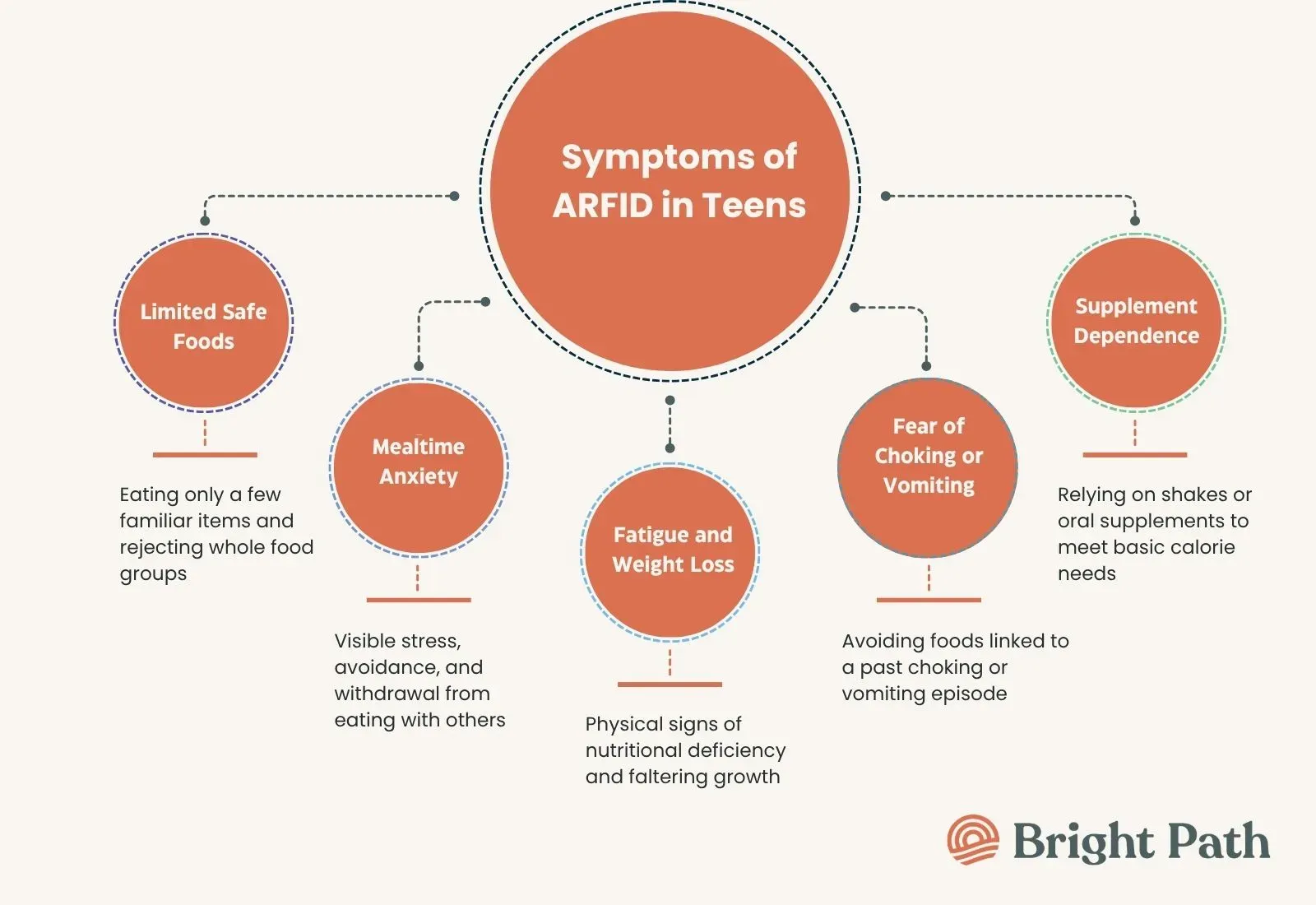
Common signs of ARFID center on a shrinking diet and rising distress around food. These behaviors usually appear long before medical symptoms emerge.
- A very limited food list: The teen eats the same few safe foods and rejects whole categories based on texture, smell, or brand.
- Mealtime anxiety and avoidance: Eating triggers visible stress, and the teen withdraws from meals with family or friends.
- Slow eating and low appetite: The teen reports little hunger, eats tiny portions, or relies on nutritional supplements to fill gaps.
Severe Symptoms of ARFID
Severe ARFID produces measurable medical harm that demands prompt clinical attention. The following warning signs call for same-day medical evaluation:
- Rapid weight loss or stalled growth: Sudden drops in weight, faltering growth, or failure to gain expected weight signal urgent nutritional risk.
- Fainting, dizziness, or a slow heart rate: These point to electrolyte imbalance or cardiovascular strain from inadequate intake.
- Dependence on tube or supplement feeding: Needing enteral nutrition or near-total reliance on oral supplements marks a severe presentation.
Long-Term Health Risks of ARFID
Untreated ARFID drives lasting damage to growth, organ systems, and emotional development. These risks accumulate the longer restriction continues.
- Nutritional deficiency diseases: Prolonged restriction produces iron deficiency anemia, vitamin C deficiency, and vitamin D deficiency that weaken the body.
- Delayed development: Chronic malnutrition contributes to stunted growth and delayed puberty during critical adolescent years.
- Deepening isolation: Persistent social withdrawal from eating erodes friendships and family connection over time.
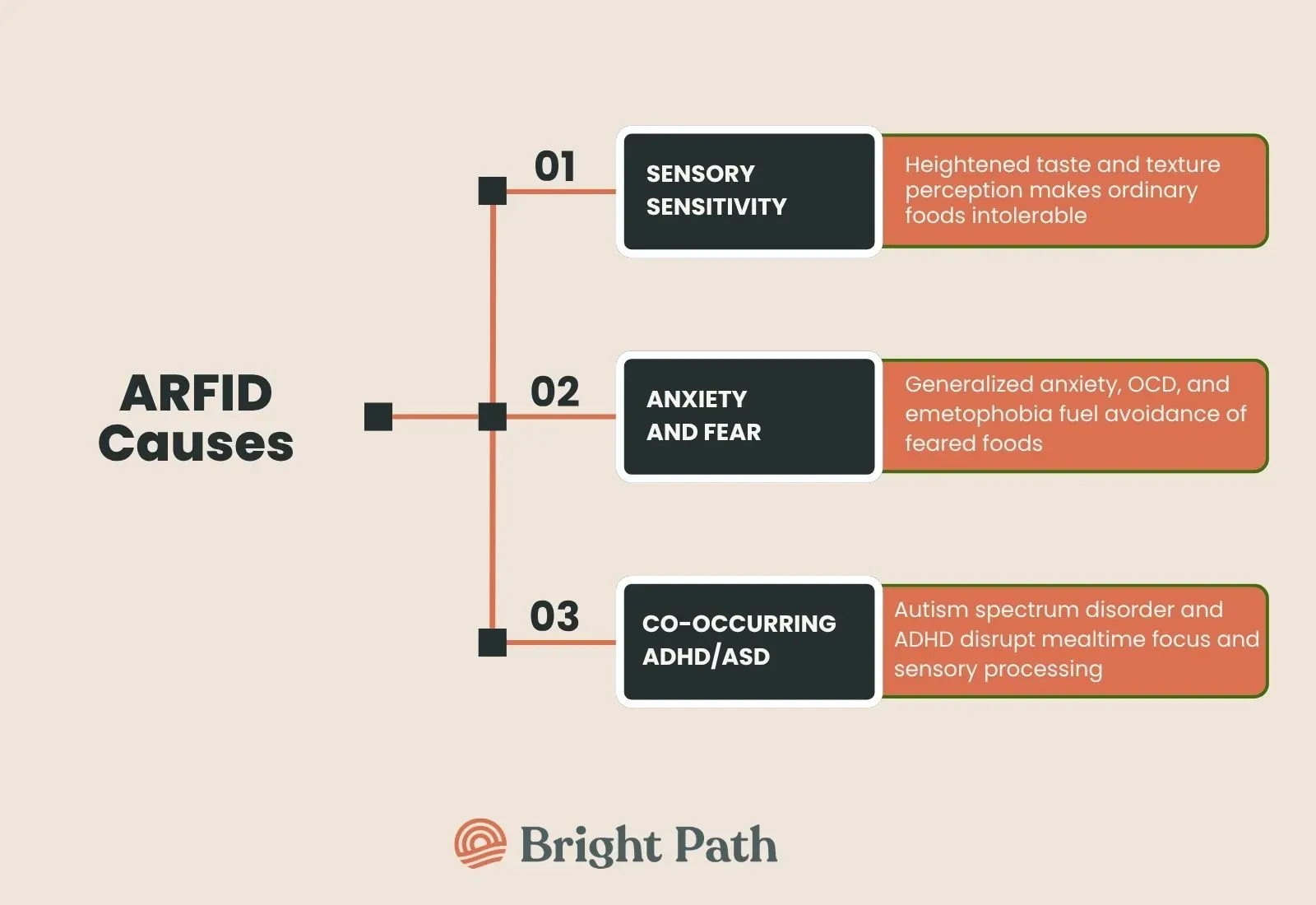
What Causes ARFID?
ARFID in adolescents grows from biological, developmental, and psychological roots rather than from a single cause. Researchers Thomas and colleagues proposed a three-dimensional neurobiological model in 2017 that maps each subtype to a distinct brain pathway. Biological differences shape how a teen's brain processes taste, appetite, and threat, which steers each ARFID subtype. ARFID frequently travels with other diagnoses, and each pairing intensifies food avoidance through its own mechanism. Anxiety disorders rank as the most common companion because fear amplifies avoidance of feared foods.
How ARFID Is Diagnosed
ARFID diagnosis relies on a structured clinical assessment that matches a teen's eating pattern to DSM-5-TR criteria while ruling out other causes. A clinician confirms that restriction causes real harm and does not stem from food scarcity, culture, or another disorder.
Validated screening tools PARDI and NIAS sharpen ARFID diagnosis by measuring the three core presentations directly. A full ARFID screening also checks bloodwork for nutritional deficiency and reviews growth charts, because medical and psychological data together confirm the diagnosis.
ARFID vs Anorexia Nervosa
ARFID and anorexia nervosa both involve severe food restriction, yet the motivation behind each disorder differs completely. Anorexia nervosa centers on body image disturbance and fear of weight gain, while ARFID does not.
Feature | ARFID | Anorexia Nervosa |
Core driver | Sensory aversion, low appetite, or fear of choking or vomiting | Fear of weight gain and pursuit of thinness |
Body image | Generally undisturbed | Distorted perception of body shape and size |
Weight goal | No desire to lose weight | Active drive to lose weight |
Common onset | Often early childhood, persisting into the teens | Most often early to mid-adolescence |
Frequent overlaps | Autism spectrum disorder, anxiety, ADHD | Anxiety, OCD, depression |
This distinction shapes care directly, because treatment that targets body image in obsessive-compulsive disorder or anorexia would miss the sensory and fear-based roots of ARFID.
How ARFID Is Treated?
ARFID treatment combines structured therapy, nutritional support, and a multidisciplinary team to widen a teen's diet safely. Care begins with the least intensive setting that keeps the teen medically stable. Nutritional rehabilitation restores missing nutrients while therapy addresses the avoidance underneath. A registered dietitian guides this process within a multidisciplinary team.
Medication plays a supporting role in ARFID because no drug holds FDA approval for the disorder itself. Clinicians may prescribe medication off-label to ease specific barriers to eating. Evidence-based therapies form the foundation of ARFID care and target the specific driver behind each teen's avoidance. Several modalities carry the strongest support.
- CBT: Cognitive behavioral therapy for ARFID gradually expands food variety through structured exposure and skill building.
- FBT: Family-based treatment trains parents to guide eating at home and rebuild regular meals.
- Graded exposure and feeding therapy: Step-by-step food exposure, often supported by occupational therapy and speech-language pathology, lowers sensory and fear responses.
Supporting a Teen With ARFID at Bright Path Behavioral Health
Bright Path Behavioral Health supports medically stable teens by treating the anxiety, sensory, and emotional drivers that often sit beneath ARFID. Bright Path uses a DBT-based model that strengthens emotional regulation and distress tolerance in teens ages 12 to 18. These skills directly target the anxiety and fear that fuel fear-based food avoidance. A teen can move from intensive day support toward a lighter after-school program as stability returns.
Frequently Asked Questions
Can a teen outgrow ARFID on its own?
ARFID rarely resolves without support once it disrupts growth or daily life. Some mild cases ease with maturity, but most teens need structured therapy to expand their diet. Early treatment lowers the chance that restriction hardens into a lasting pattern with medical complications.
Is ARFID more common in boys or in girls?
ARFID appears more evenly distributed between boys and girls than most eating disorders. Several studies report it is more common in boys than anorexia nervosa is. This balance partly reflects its strong link to autism spectrum disorder, which is diagnosed more often in boys.
Can a teen have ARFID and anorexia nervosa at the same time?
A teen cannot hold both diagnoses simultaneously, because the criteria exclude each other. However, a small number of teens shift from ARFID to anorexia nervosa over time if body image concerns later emerge. A clinician reassesses the diagnosis whenever the motivation behind restriction changes.
Can adults develop ARFID?
Yes, adults can develop ARFID, even though it often begins in childhood or the teen years. Untreated childhood ARFID frequently persists into adulthood. Recognition in adults has grown as awareness of the diagnosis spreads beyond pediatric settings.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). American Psychiatric Publishing.
- Thomas, J. J., Lawson, E. A., Micali, N., Misra, M., Deckersbach, T., & Eddy, K. T. (2017). Avoidant/restrictive food intake disorder: A three-dimensional model of neurobiology with implications for etiology and treatment. Current Psychiatry Reports, 19(8), 54. >
- Bryant-Waugh, R., Micali, N., Cooke, L., Lawson, E. A., Eddy, K. T., & Thomas, J. J. (2019). Development of the Pica, ARFID, and Rumination Disorder Interview (PARDI). International Journal of Eating Disorders, 52(4), 378–387.
- Zickgraf, H. F., & Ellis, J. M. (2018). Initial validation of the Nine Item Avoidant/Restrictive Food Intake Disorder Screen (NIAS). Appetite, 123, 32–42. >
- Sanchez-Cerezo, J., Neale, J., Julius, N., Croudace, T., Lynn, R. M., Hudson, L. D., & Nicholls, D. (2024). Subtypes of avoidant/restrictive food intake disorder in children and adolescents: A latent class analysis. eClinicalMedicine, 68, 102440.
- Eddy, K. T., Thomas, J. J., Hastings, E., Edkins, K., Lamont, E., Nevins, C. M., et al. (2015). Prevalence of DSM-5 avoidant/restrictive food intake disorder in a pediatric gastroenterology healthcare network. International Journal of Eating Disorders, 48(5), 464–470.
- National Institute of Mental Health. (2023). Eating disorders: About more than food. U.S. Department of Health and Human Services.>
- Zimmerman, J., & Fisher, M. (2017). Avoidant/restrictive food intake disorder (ARFID). Current Problems in Pediatric and Adolescent Health Care, 47(4), 95–103.