Delusional disorder is characterized by the presence of one or more delusions—false beliefs that persist despite evidence to the contrary. This disorder is relatively rare, affecting approximately 0.2% of the population, and emerges in middle to late adulthood, according to a study by professional psychiatrist Shawn M., et al published in StatPearls in 2023 titled “Delusional Disorder.”
The main symptoms of delusional disorder include persistent beliefs that vary widely, encompassing everything from paranoid thoughts—where individuals feel they are being persecuted or conspired against—to grandiose ideas, which involve an inflated sense of self-importance or extraordinary abilities. These delusions are well-formed, detailed and consistent, leading individuals to construct elaborate narratives around their beliefs.
The types of delusional disorder include the persecutory type, where individuals believe they are being targeted or harassed; the grandiose type, characterized by beliefs in exceptional abilities or fame; the jealous type, involving convictions of a partner’s infidelity; erotomanic type, where one believes someone is in love with them; and somatic type, which relates to false beliefs about bodily sensations or functions.
The causes of delusional disorder are family history of mental illness, stressful life events, and certain medical conditions that can affect mental health. Diagnosis for the disorder involves a comprehensive clinical assessment, including a psychiatric evaluation to distinguish delusional disorder from other mental health issues.
Treatment for delusional disorder options primarily include antipsychotic medications and psychotherapy. The efficacy of these treatments varies; some individuals experience improvement while others continue to struggle with persistent delusions despite intervention. Close to half of patients treated with antipsychotic medications show at least partial improvement , per a study by the WebMD Editorial Contributors published in WebMD in 20234 titled “Delusional Disorder: Types, Symptoms, and Treatment.”
The prognosis for individuals with delusional disorder is quite variable. Some achieve remission, while others might continue to experience delusions over time. Moreover, delusional disorder can be associated with other mental health conditions, such as schizophrenia or mood disorders, which can complicate treatment and recovery.
What is Delusional Disorder?
Delusional disorder is a type of mental disorder that includes the presence of one or more delusions that persist for at least one month. These delusions are fixed false beliefs that are not based on reality and significantly impair an individual’s ability to function in daily life. Core characteristics of delusional disorder include the presence of well-formed delusions, which are paranoid (believing one is being persecuted), grandiose (having an inflated sense of self-importance), jealous (believing a partner is unfaithful), erotomanic (assuming someone is in love with them), or somatic (having false beliefs about bodily sensations).
People with delusional disorder generally maintain a level of functioning that is not markedly impaired aside from the delusions, and their behavior appears normal outside the context of their beliefs. Also, they experience poorer sight and greater general psychopathology compared to those with schizophrenia, although their social functioning is similar, as found by a comparative study, by Christy L. M. PhD., et al published in BMC Psychiatry in 2023 titled “Functional and clinical outcomes of delusional disorder and schizophrenia patients after first-episode psychosis: a 4-year follow-up study.”
Delusional disorder was first recognized in the late 19th century, with its roots in early psychiatric classifications of psychotic disorders. While early descriptions of psychotic conditions included various forms of delusional thinking, it wasn’t until the development of structured diagnostic criteria in the 20th century that delusional disorder became formally defined within psychiatric literature. Its identification has evolved alongside our understanding of mental disorders, reflecting ongoing advances in the field of psychology and psychiatry.
How Common is Delusional Disorder?
Delusional disorder is considered a rare mental health condition. Prevalence data indicates that the lifetime prevalence of the delusional disorder in the general population is estimated to be around 0.02% according to the DSM-5. In the United States, the prevalence is similarly low, with estimates aligning closely with the DSM-5 figures. Among patients presenting with a first episode of psychosis, approximately 7% were diagnosed with persistent delusional disorder, which highlights its relative rarity compared to other psychotic disorders such as schizophrenia., as reported by a British study published in Medscape in 2022 titled Delusional Disorder.
Demographic trends indicate that delusional disorder affects individuals across various age groups, but it is more commonly diagnosed in middle to late adulthood. The same study published in Medscape mentioned that the mean age of onset is around 40 years, with a range extending from 18 to 90 years. Gender differences have also been noted, the female-to-male ratio is approximately 1.18 to 3:1, indicating that women are more likely to develop certain types of delusions, such as erotomanic delusions, while men are more prone to paranoid delusions.
Several risk factors have been identified for delusional disorder. These include a family history of mental illness, which increases susceptibility, as well as stressful life events that trigger the onset of delusions. Additionally, some medical conditions, particularly those affecting the brain, also contribute to the development of delusional disorder.
Older adults, particularly women, are at a higher risk for developing delusional disorder, possibly due to age-related changes in brain function and increased vulnerability to stressors.
At What Age Does Delusional Disorder Start?
Delusional disorder most commonly presents in late adolescence to early adulthood, with a mean onset age of around 40 years, although it varies among individuals.
Some individuals start to exhibit symptoms as early as 18, while many cases are diagnosed in their 20s and 30s. A significant number of diagnoses occur in middle adulthood, particularly in individuals in their 40s and 50s. Different subtypes of delusional disorder have varying onset ages; for example, paranoid delusions are seen in middle-aged individuals, while erotomanic delusions appear more frequently in younger adults.
This disorder involves a gradual increase in symptoms over several months or years, rather than a sudden onset, complicating early identification.
Can Kids Have Delusional Disorder?
Yes, children can experience delusional disorder, although it is relatively rare. When delusional disorder manifests in children, it presents differently than in adults. The prevalence of childhood-onset psychosis, including delusional disorder, is estimated to be about 0.0025% for childhood-onset schizophrenia.
In children, the delusions are less complex and are sometimes mistaken for imaginative play or typical childhood fantasies.
However, the key distinguishing feature is that the beliefs held by the child are firmly entrenched and not influenced by reality, which leads to significant distress or impairment in functioning.
In children, delusions manifest as beliefs that are more concrete and less elaborate than those seen in adults. For example, a child might believe that they have superpowers or that they are being watched by a specific character from a show. These beliefs lead to social withdrawal, difficulties in school, and strained family relationships. Additionally, children do not have the insight to recognize that their beliefs are not based on reality, which complicates diagnosis and treatment.
What Are the Symptoms of Delusional Disorder?
The symptoms of delusional disorder are delusions, social withdrawal, anxiety, depression, and irritability. These symptoms significantly affect a person’s thoughts, emotions, and behaviors. The main symptoms are categorized into cognitive and behavioral symptoms.
These symptoms lead to significant distress and impairment in various aspects of life, making early diagnosis and intervention crucial for effective treatment.
How Does Delusional Disorder Impact Daily Life?
Delusional disorder impacts daily life, affecting various aspects such as functioning, relationships, and work life. Individuals struggle with maintaining employment due to their delusions, which lead to difficulties in concentration and decision-making. For example, someone with paranoid delusions believes that coworkers are conspiring against them, leading to increased anxiety and withdrawal from social interactions.
In personal relationships, delusions create mistrust and conflict; a person with jealous delusions accuses their partner of infidelity without any evidence, straining the relationship. Also, the persistent nature of these delusions leads to social isolation, as individuals avoid situations where they feel their beliefs could be challenged or ridiculed.
Do People with Delusional Disorder Have Hallucinations?
No, individuals with delusional disorder do not experience hallucinations as a core symptom. Delusional disorder is primarily characterized by the presence of delusions, which are fixed false beliefs that are not based on reality. In contrast, hallucinations involve sensory experiences that occur without an external stimulus, such as hearing voices or seeing things that are not there.
While hallucinations and delusions are both symptoms of psychosis, they differ fundamentally: delusions are cognitive distortions, whereas hallucinations are sensory perceptions. Although hallucinations co-occur with delusions in some cases, particularly in more severe forms of psychosis like schizophrenia, they are not a defining feature of delusional disorder itself, says a 2024 study by researcher, Sanjana G., published in Verywell Mind 2024 titled “Delusions versus Hallucinations: What Are the Differences?.”
Can a Delusional Disorder Cause Anger or Hostility?
Yes, delusional disorder leads to anger or hostility in individuals. Behavioral manifestations include irritability and increased agitation, particularly when the person feels that their delusions are being challenged or dismissed. For example, a person experiencing paranoid delusions reacts with hostility toward others whom they perceive as threats, believing that they are being persecuted or targeted.
Potential triggers for this anger include perceived insults, challenges to their beliefs, or stressors in their environment. The emotional turmoil associated with maintaining these delusions also contributes to an overall sense of frustration and defensiveness, leading to aggressive outbursts or withdrawal from social interactions.
Can You Be Aware of Delusions?
Yes, some people with delusional disorders are aware of their delusions. This awareness, known as “insight,” varies significantly among individuals. While some recognize that their beliefs are irrational or not grounded in reality, others firmly believe in the validity of their delusions despite evidence to the contrary.
Those with better insight experience internal conflict, feeling distressed by their beliefs even while holding onto them. This awareness influences their willingness to seek treatment and their overall functioning.
What Are Different Types of Delusional Disorder?
The different types of delusional disorder are erotomanic, grandiose, jealous, persecutory, somatic, and mixed delusions, according to a systematic review published in Frontiers in 2022 titled “Clinical and Structural Differences in Delusions Across Diagnoses: A Systematic Review.” These types of delusional disorders are explained below:
1. Erotomanic Type: Eromatic delusion involves the belief that another person, of higher social status, is in love with the individual. A common example is someone who believes that a celebrity has romantic feelings for them, leading them to engage in behaviors such as sending letters or gifts in an attempt to establish a connection.
2. Grandiose Type: Individuals with grandiose delusions have an inflated sense of self-importance or believe they possess exceptional abilities, talent, or fame. For instance, a person might believe they are a famous artist or that they have discovered a groundbreaking scientific principle, leading them to dismiss the opinions of others.
3. Jealous Type: The jealous delusion is characterized by the belief that a partner is being unfaithful. Individuals exhibit behaviors such as stalking or interrogating their partner about their whereabouts. Common manifestations include constant suspicion and unfounded accusations that lead to significant relationship turmoil.
4. Persecutory Type: Individuals with persecutory delusions believe that they are being targeted, harassed, or conspired against by others. Signs include expressing fears of being followed, monitored, or harmed by specific individuals or organizations, leading to social withdrawal and heightened anxiety.
5. Somatic Type: Somatic delusion involves delusions related to bodily functions or sensations. For example, an individual believes they have a serious medical condition despite medical evaluations showing no evidence of illness, such as believing they are infested with parasites or that their organs are malfunctioning.
6. Mixed and Unspecified Types: In mixed types, individuals experience delusions from more than one category without a dominant theme, leading to a combination of symptoms. Unspecified types refer to cases where the delusions are present but do not fit neatly into the defined categories, making diagnosis and treatment more complex.
What Is the Most Common Type of Delusion?
The most common type of delusion is the persecutory delusion. This type involves the belief that one is being targeted, harassed, or conspired against by others, despite a lack of evidence to support such claims. Individuals experiencing persecutory delusions feel that they are being spied on, followed, or harmed by others, which leads to significant distress and impairment in their daily lives.
Persecutory delusions are prevalent among various psychiatric disorders, particularly in conditions like schizophrenia and delusional disorder. Over 70% of patients experiencing their first episode of psychosis report having persecutory delusions, as indicated in a review by psychiatrist Daniel. F., et al published in Springer in 2014 titled “Advances in understanding and treating persecutory delusions.”
What Is Shared Delusional Disorder?
Shared delusional disorder, also known as folie à deux, is a rare psychiatric condition characterized by the sharing of a delusion between two or more individuals who are in a close relationship. One person (the “primary”) has a psychotic disorder that includes delusions, and this individual influences another person (the “secondary”) to adopt their false beliefs, according to research by Feras. A., et al published in StatPearls in 2023 titled “Shared Psychotic Disorder.”
The exact causes of shared delusional disorder are not fully understood, but several factors like close relationships, social isolation, and stressful life events contribute to its development.
What Causes Delusional Disorder?
Delusional disorder is caused by genetic factors, neurobiological factors, and environmental factors. Understanding these factors helps in identifying and treating the disorder effectively. Here are the primary causes of delusional disorder:
- Genetic factors: Individuals with a family history of psychotic disorders, including schizophrenia, have a higher risk of developing delusions. Genetic studies suggest that certain genes associated with neurotransmitter systems, particularly dopamine, influence susceptibility to psychotic disorders, including delusional disorders.
- Neurobiological factors: Neurobiological factors, particularly those related to brain structure and function, are important in understanding delusional disorders. Abnormalities in brain regions such as the prefrontal cortex and temporal lobes, which are involved in perception and reality testing, have been linked to the disorder. Additionally, dysregulation of neurotransmitters, especially dopamine, is thought to contribute to the formation of delusions.
- Environmental factors: Environmental influences, including stressful life events, trauma, and social isolation, trigger or exacerbate delusional disorder. Individuals who experience significant stress, such as the loss of a loved one or prolonged social isolation, are more vulnerable to developing delusions. Furthermore, exposure to substance use, particularly alcohol, also plays a role. Alcohol use disorder is known to co-occur with various psychiatric conditions, and heavy drinking leads to cognitive impairments and altered perceptions, which contribute to the onset of delusional beliefs.
How Does Delusional Disorder Develop?
Delusional disorder develops gradually, with symptoms emerging over time rather than appearing suddenly. The progression is understood in several stages, beginning with the initial onset and evolving into more established cases.
In the early stage, individuals experience mild, transient symptoms, such as unusual thoughts or perceptions that do not yet qualify as delusions. During this phase, they feel a heightened sense of suspicion or awareness about their surroundings while maintaining some insight into their thoughts. They recognize these thoughts as odd but do not fully believe them.
As the disorder progresses to the emerging stage, the delusions become more pronounced. Individuals fixate on specific beliefs related to themes of persecution or grandiosity. At this point, these delusions start to interfere with daily life as the person begins to act on these beliefs.
In the established stage, the delusions become entrenched and resistant to reason. Individuals experience significant impairment in social, occupational, and personal functioning. Their insight diminishes, leading them to firmly believe in the validity of their delusions despite evidence to the contrary. Relationships suffer as paranoia or grandiosity escalates, resulting in conflicts with family, friends, and coworkers. Additionally, individuals experience associated symptoms such as anxiety and depression, further complicating their emotional state.
What Are the Risk Factors for Delusional Disorder?
The risk factors for delusional disorder include family history, trauma, social isolation, substance abuse, and chronic stress. They are explained below:
- Family history: A genetic predisposition to psychotic disorders, including schizophrenia, increases the likelihood of developing delusional disorder.
- Trauma: Experiencing significant life stressors or traumatic events, such as loss, abuse, or violence, triggers or exacerbates delusional symptoms.
- Social isolation: Individuals who are socially isolated or lack supportive relationships are more vulnerable to developing delusions, as they have limited exposure to differing perspectives.
- Substance use: Alcohol and drug abuse impair judgment and perception, potentially leading to the onset of delusional beliefs.
- Chronic stress: Prolonged exposure to stress, whether from personal, financial, or environmental factors, contributes to the development of delusional disorder.
What Triggers Delusional Disorder?
The specific triggers that worsen symptoms of delusional disorder include stressful life events, environmental stressors, changes in routine, loss of control, and exposure to misinformation.
- Stressful life events: Major changes or stressors, such as the death of a loved one, divorce, job loss, or significant financial difficulties, trigger or worsen delusional beliefs.
- Environmental stressors: Factors such as living in a chaotic or unsafe environment, experiencing ongoing conflict, or facing discrimination contribute to the exacerbation of delusional symptoms.
- Changes in routine: Disruptions to daily routines or significant lifestyle changes create feelings of instability, potentially triggering delusional thoughts.
- Loss of control: Situations that lead to a perceived loss of control, such as health crises or sudden changes in personal circumstances, heighten feelings of anxiety and contribute to delusional thinking.
- Exposure to misinformation: Consuming unreliable information or being surrounded by individuals who reinforce delusional beliefs exacerbates existing symptoms and leads to further entrenchment of delusions.
Understanding these triggers is important for managing delusional disorders and developing strategies to mitigate the impact of these stressors on individuals’ mental health.
Can PTSD Cause Delusional Disorder?
Yes, PTSD can cause delusional disorder, particularly in terms of comorbidity. The trauma associated with PTSD leads to significant alterations in cognition there and perception, which contribute to the emergence of delusional beliefs.
A 68-year-old man who, after losing his family in a traumatic event, developed PTSD with psychotic features. He exhibited delusional beliefs that his family was still alive and suffered persistent hallucinations, reflecting how extreme trauma leads to psychosis-like symptoms, per a case report published by BMJ Case in 2021 titled “Psychotic PTSD? Sudden traumatic loss precipitating very late-onset schizophrenia.”
PTSD is underdiagnosed in patients with schizophrenia and related disorders, with a study published in Progress in Neuro-Psychopharmacology & Biological Psychiatry in 2020 titled “Posttraumatic Stress Disorder with Secondary Psychotic Features (PTSD-SP): Diagnostic and Treatment Challenges” showing that approximately 30% of individuals with schizophrenia spectrum disorders also meet the criteria for PTSD. This overlap highlights the complexity of diagnosing and treating individuals who present with both PTSD and delusional disorder.
Does Delusional Disorder Get Worse With Age?
Yes, delusional disorder (DD) worsens with age, although the severity varies among individuals. As people age, delusions become more entrenched, influenced by cognitive decline, social isolation, and comorbid health issues. Older adults experience increased rigidity in their delusional beliefs, making them less likely to change. Cognitive decline exacerbates these delusions, as impairments in memory and executive functioning hinder critical evaluation of beliefs.
Women are more vulnerable to developing DD in old age, particularly postmenopause. Of 80 women with DD, 55 had postmenopausal onset, suggesting a link between age and the disorder’s onset, according to a prospective observational study by Alexandre G., et al published in the International Journal of Environmental Research and Public Health in 2022 titled “Delusional Disorder in Old Age: A Hypothesis-Driven Review.”
The content of delusions shifts with age; older adults develop non-bizarre delusions related to health concerns or beliefs about being mistreated. Increased life stressors, such as bereavement, also trigger or worsen delusions. Additionally, comorbid conditions like depression and anxiety are common in older adults with DD, further exacerbating symptoms and leading to poorer outcomes. Treatment responses are complicated by more pronounced side effects from antipsychotic medications in this population, impacting symptom management.
How Is Delusional Disorder Diagnosed?
Delusional disorder (DD) is diagnosed by implementing the DSM-5 criteria and specific assessment tools. The primary source for diagnosing DD is the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Key criteria include the presence of one or more delusions lasting at least one month, which must not be better explained by another mental disorder (e.g., schizophrenia). Additionally, functioning outside the delusion should not be markedly impaired, and the episode must not be attributable to a medical condition or substance use.
A detailed clinical assessment is also necessary for diagnosis. This involves a comprehensive clinical interview to gather information about the patient’s history, symptoms, and overall functioning. During this interview, practitioners ask questions about the nature of the delusions and their impact on daily life. Similarly, a mental status examination is performed to evaluate cognitive function, appearance, mood, and thought processes, helping to identify signs of delusions and other psychological issues.
Standardized assessment tools are used to further support the diagnosis. Psychometric tests, such as the Positive and Negative Syndrome Scale (PANSS), assess the severity of symptoms, while structured interviews, like the Structured Clinical Interview for DSM Disorders (SCID), ensure a thorough evaluation based on DSM criteria.
Gathering collateral information is another important aspect of the diagnostic process. Information from family members or caregivers provides additional context regarding the patient’s behavior and beliefs, aiding in the diagnosis.
Finally, it is essential to rule out other mental health disorders and medical conditions that could explain the symptoms. This ensures an accurate diagnosis of delusional disorder, allowing for appropriate treatment and management of the condition.
Diagnostic Process for Delusional Disorder
The diagnostic process for DD involves careful evaluation based on established criteria from the DSM-5, along with considerations for differential diagnosis to ensure accurate identification of the disorder.
DSM-5 Criteria for Delusional Disorder
According to the DSM-5, the diagnosis of delusional disorder requires the following criteria:
- Presence of delusions: The individual must have one or more delusions that persist for at least one month.
- Functioning: Apart from the delusions, the individual’s functioning is not markedly impaired, and behavior is not bizarre or odd. This distinguishes DD from other psychotic disorders, where functioning is more disrupted.
- Duration: The episode of delusions must last for at least one month. If the delusions are part of a brief psychotic episode, the diagnosis will be different.
- Exclusion of other disorders: The delusions must not be better explained by another mental disorder, such as schizophrenia or a mood disorder with psychotic features. If the symptoms occur during a mood disorder, the diagnosis of DD is not made.
- Substance use or medical condition: The delusions must not be attributable to the physiological effects of a substance (e.g., drug abuse, medication) or another medical condition (e.g., a head injury or a neurological disorder).
Differential diagnosis is critical in distinguishing delusional disorder from other psychiatric conditions that present with similar symptoms. Key considerations include:
- Schizophrenia: Schizophrenia involves more pervasive symptoms, including hallucinations, disorganized thinking, and negative symptoms. If the individual has experienced hallucinations or significant functional impairment beyond the delusions, a diagnosis of schizophrenia is warranted.
- Mood disorders with psychotic features: In cases where delusions occur during episodes of major depression or bipolar disorder, the diagnosis shifts to a mood disorder with psychotic features. The key distinction is that the mood disorder symptoms are dominant.
- Substance-induced psychotic disorder: If delusions are a direct result of substance use or withdrawal, the diagnosis should reflect that. It is essential to determine whether the delusions occurred during intoxication or withdrawal from substances.
- Medical conditions: Certain medical conditions, such as neurological disorders (e.g., dementia, seizures) or endocrine disorders (e.g., hyperthyroidism), produce psychotic symptoms. A thorough medical evaluation is necessary to rule out these underlying conditions.
- Paranoid personality disorder: Individuals with paranoid personality disorder exhibit persistent distrust and suspicion but do not have fixed delusions. The beliefs of paranoid personality disorder are more flexible and do not meet the criteria for delusions.
Common Tests for Delusional Disorder
Common tests for delusional disorder include psychiatric evaluations, imaging studies, blood tests, and neuropsychological testing. These tests are aimed at ruling out other conditions and confirming the diagnosis. Here are some of the key tests used in the diagnostic process:
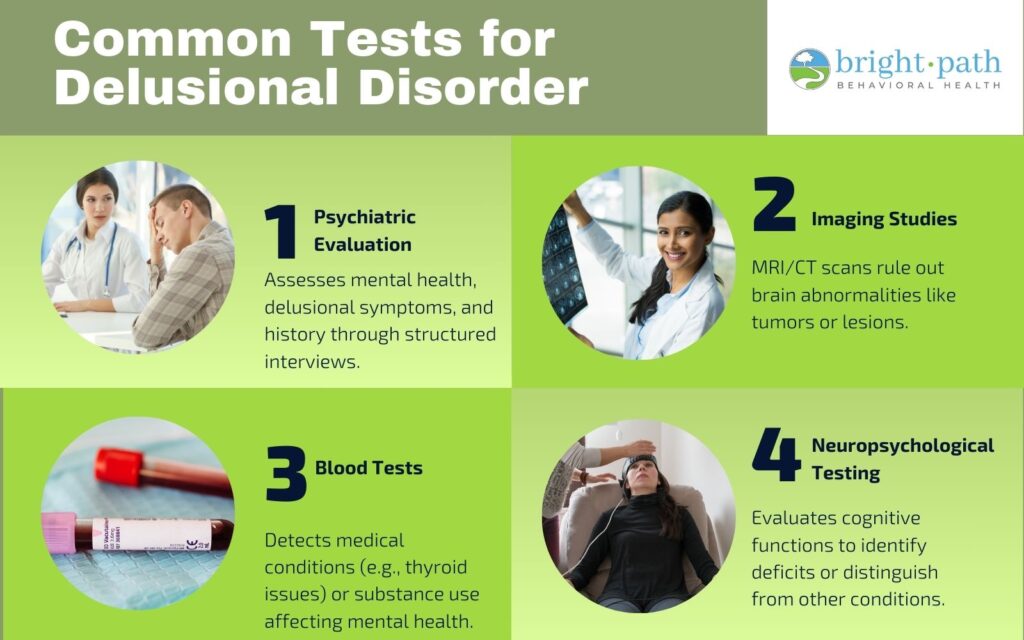
- Psychiatric Evaluations: Comprehensive interviews and assessments are conducted to gather detailed information about the patient’s history, symptoms, and functioning. This includes evaluating the content and duration of delusions, any associated mood symptoms, and overall mental health. Structured interviews, such as the Structured Clinical Interview for DSM Disorders (SCID), are used to ensure adherence to diagnostic criteria.
- Imaging Studies: Imaging studies, specifically MRI and CT scans, are important diagnostic tools used to evaluate brain structure and rule out underlying conditions that could contribute to psychiatric symptoms, including delusions. MRI (Magnetic Resonance Imaging) provides detailed images of the brain’s structure, allowing for detecting abnormalities such as tumors, lesions, and neurodegenerative diseases. CT (Computed Tomography) scans are another method used to identify structural brain issues, helping to detect strokes and significant brain atrophy associated with various psychiatric disorders.
- Blood Tests: Routine blood tests are essential for ruling out medical conditions that might cause or worsen psychotic symptoms. These tests help identify physiological factors that could be contributing to the individual’s mental state. Thyroid function tests assess hormone levels to determine if the thyroid is underactive (hypothyroidism) or overactive (hyperthyroidism), both of which significantly affect mood and cognition. A complete blood count (CBC) provides information on overall health, helping to identify infections or hematological issues that lead to psychological symptoms. Metabolic panels evaluate kidney and liver function, as well as electrolyte balance, which can impact mental status and lead to symptoms resembling psychosis. Toxicology screens detect the presence of drugs or alcohol in the system, as substance use significantly influences an individual’s mental state and mimics or exacerbates delusional symptoms.
- Neuropsychological Testing: These assessments measure cognitive function, including memory, attention, and executive functioning. Such tests help identify cognitive deficits that are associated with delusional disorder or other mental health conditions.
What Are Treatment Options for Delusional Disorder?
The treatment options for DD are medications, psychotherapy, alternative treatments, and support systems. This general approach to therapy focuses on alleviating symptoms, improving functioning, and enhancing the quality of life for individuals affected by this disorder.
1. Medications
Medications are the first line of treatment for delusional disorder, primarily focusing on antipsychotic medications.
- Antidepressants: Antidepressants are sometimes prescribed if the individual with DD also experiences depressive symptoms. Common options include SSRIs like fluoxetine, which help improve mood but have side effects such as gastrointestinal upset or sexual dysfunction.
- Mood Stabilizers: Medications like lithium or valproate are used in cases where mood swings are present alongside delusions.
The best medication for delusional disorder is Clozapine because it has demonstrated superior efficacy in managing symptoms of delusional disorder compared to other antipsychotics, especially in treatment-resistant cases, says a 2022 study by Mental Health Specialist, Alexandre G., et al published in Biomedicines MDPI titled “Seventy Years of Treating Delusional Disorder with Antipsychotics: A Historical Perspective.”
2. Psychotherapy
In conjunction with medication, psychotherapy helps in the treatment of delusional disorder. Different types of psychotherapy treatments to consider include:
- Cognitive Behavioral Therapy (CBT): When CBT is adapted for psychosis, it helps individuals with delusions (false beliefs) and hallucinations (perceptions that aren’t real). It focuses on changing how they think about and respond to these experiences, aiming to reduce their distress and improve daily functioning, according to a research published by Child Mind Institute in 2024 titled “How Does CBT Help People With Psychosis?”
- Supportive Therapy: This approach provides emotional support and helps individuals cope with their symptoms. It does not directly challenge delusions but improves the therapeutic relationship and provides a safe space for expression.
3. Alternative Treatments
Alternative therapies complement traditional treatment methods, although their effectiveness varies. Common types of alternative treatments include:
- Mindfulness and Meditation: These practices help reduce anxiety and improve overall mental well-being, though they do not directly address delusions.
- Support Groups: Connecting with others who have similar experiences provides emotional support and reduces feelings of isolation.
- Holistic Practices: Approaches such as yoga or acupuncture promote relaxation and stress relief, but scientific evidence supporting their effectiveness for delusional disorders is limited.
4. Self-Management and Support Systems
Self-management strategies and support systems are vital for individuals with delusional disorders. Some self-management strategies include:
- Lifestyle Adjustments: Regular exercise, a balanced diet, and adequate sleep improve overall mental health and resilience.
- Education: Learning about the disorder empowers individuals and their families, helping them understand symptoms and treatment options.
- Support Groups: Engaging with support groups provides a sense of community and shared therapeutic experience.
Can Delusional Disorder Be Cured?
No, delusional disorder cannot be cured, but it is effectively managed. Current perspectives on treatment outcomes suggest that many individuals experience significant symptom relief and improved functioning through a combination of medications and psychotherapy.
Remission possibilities vary; some people achieve full remission of symptoms, while others have persistent delusions that are managed over time. With appropriate treatment, many individuals lead fulfilling lives, but ongoing support and monitoring are necessary to maintain stability and address any recurring symptoms.
What Is the Outlook for Individuals with Delusional Disorder?
The outlook for individuals with delusional disorder is positive, especially when they adhere to their treatment plans. Approximately 50% of individuals achieve a full recovery, while over 20% experience a reduction in their symptoms. Conversely, less than 20% report minimal to no change in their condition, based on a study by Cleveland Clinic in 2022 titled “Delusional Disorder.”
Many people respond positively to treatment, particularly when a combination of antipsychotic medications and psychotherapy, such as cognitive behavioral therapy (CBT), is used. Some patients achieve significant symptom relief and many experience improvements in daily functioning and quality of life. Full remission is possible for some, but others continue to experience persistent delusions that require ongoing management.
One of the primary challenges in treating delusional disorder is the nature of the delusions themselves. Individuals are resistant to accepting that their beliefs are unfounded, which hinders treatment adherence. Also, the stigma associated with mental health disorders leads to social isolation, further complicating recovery.
The duration of delusional disorder varies. Some episodes last for a few months, while others persist for years. If left untreated, delusional disorder becomes chronic, with symptoms that fluctuate in intensity over time. Early intervention and consistent treatment help reduce the duration and severity of symptoms, improving the overall prognosis for individuals affected by the disorder.
How to Live with Delusional Disorder?
To live with delusional disorder, people with DD need to follow treatment plans, establish a routine, practice self-care, develop coping strategies, communicate openly, and educate others.
Here is how to live with DD:
- Follow treatment plans: Stick to prescribed medication and therapy schedules to manage symptoms effectively. Regular check-ins with healthcare providers help adjust treatment as needed.
- Establish a routine: Create a daily routine that includes structure and stability. This helps reduce anxiety and improve overall functioning.
- Practice self-care: Engage in regular physical activity, maintain a balanced diet, and ensure adequate sleep. These factors contribute to overall mental well-being.
- Develop coping strategies: Identify personal coping mechanisms that work best for managing stress and anxiety. Techniques such as mindfulness, deep breathing, or journaling are beneficial.
- Communicate openly: Share your experiences with trusted friends or family members. Open communication fosters understanding and reduces feelings of isolation.
- Educate others: Help friends and family understand delusional disorder to combat stigma. Providing information promotes empathy and support.
How to Help Someone With Delusional Disorder?
To help someone with a delusional disorder, family and friends need to learn to listen actively, avoid confrontations, encourage treatment, be patient, create a safe space, and generally provide support with empathy and patience. Here are some effective ways to offer assistance:
- Allow them to express their feelings and thoughts without judgment. Show that you are there to listen and understand.
- Acknowledge their emotions, even if you disagree with their beliefs. This helps them feel heard and respected.
- Refrain from arguing about the delusions. Instead, focus on their feelings and experiences, which help maintain open communication.
- Gently suggest they stick to their treatment plan and attend therapy sessions. Offer to help them find resources or accompany them if they need support.
- Understand that recovery is a slow process. Offer consistent support, even when progress seems minimal.
- Learn about delusional disorder to better understand what your loved one is experiencing. This knowledge helps you provide informed support.
By following these strategies, you provide meaningful support to a loved one with a delusional disorder, fostering a positive environment for their recovery.
How to Talk to Someone With Delusional Disorder?
To talk to someone with a delusional disorder, you have to remain calm and composed, ask open-ended questions, focus on shared experiences, don’t make assumptions about their thoughts, etc. The specific strategies you need to talk to someone with a delusional disorder include:
- Maintain a gentle tone and a relaxed demeanor to create a safe environment for conversation.
- Acknowledge their emotions and experiences, even if their beliefs seem irrational. Use phrases like, “I can see this is very important to you.”
- Encourage them to express themselves by asking questions that invite deeper discussion, such as “Can you share more about what you’re experiencing?”
- Shift the conversation towards neutral topics or mutual interests to help ground the discussion in reality.
- If you feel overwhelmed, try to keep those feelings in check to avoid escalating the situation.
- Instead of assuming you know how they feel, ask questions to better understand their perspective.
By following these strategies, you engage in supportive and constructive conversations with someone who has a delusional disorder, fostering understanding and respect.
Comparisons of Delusional Disorder with Other Mental Health Conditions
Delusional disorder is compared with other mental health like schizophrenia, bipolar disorder, paranoid personality disorder, and major depressive disorder with psychotic features. Understanding the distinctions between them is important for accurate diagnosis and effective treatment. Misdiagnosis leads to inappropriate treatment plans, which do not address the specific needs of the individual.
Commonly compared disorders include:
- Schizophrenia: While both conditions involve delusions, schizophrenia includes additional symptoms such as hallucinations, disorganized thinking, and negative symptoms (e.g., lack of motivation). The delusional disorder primarily features persistent delusions without the broader range of symptoms seen in schizophrenia, as highlighted by a research assistant, Kelly R., et al in a 2022 research published in Frontiers titled “Clinical and Structural Differences in Delusions Across Diagnoses: A Systematic Review.”
- Bipolar Disorder: In bipolar disorder, delusions occur during manic or depressive episodes, but they are mood-congruent (related to the individual’s emotional state). In contrast, delusional disorder features persistent delusions that are not necessarily tied to mood fluctuations.
- Major Depressive Disorder with Psychotic Features: This condition involves depressive symptoms along with delusions or hallucinations. The key difference is that the psychotic features are secondary to the mood disorder, while in delusional disorder, the delusions are the primary issue.
- Paranoid Personality Disorder: Individuals with paranoid personality disorder exhibit distrust and suspicion, but their beliefs do not reach the level of fixed delusions seen in delusional disorder. The latter involves a more profound conviction in false beliefs despite contrary evidence.
What Is the Difference Between Delusional Disorder and Schizophrenia?
This table outlines the difference between delusional disorder and schizophrenia:
Can delusional disorder turn into schizophrenia? Yes, while delusional disorder and schizophrenia are distinct conditions, some individuals with delusional disorder later develop symptoms of schizophrenia. This progression is not common but occurs, particularly if the delusional disorder remains untreated.
Is Delusional Disorder a Personality Disorder?
No, delusional disorder is not classified as a personality disorder. Delusional disorder is characterized by the presence of persistent delusions that are not attributable to other mental health conditions. These delusions last for at least one month and are non-bizarre, meaning they involve believable scenarios, such as themes of persecution or grandiosity. Individuals with delusional disorder do not usually exhibit significant mood symptoms, hallucinations, or disorganized thinking, which are common in schizophrenia.
In contrast, personality disorders involve enduring patterns of behavior, cognition, and inner experiences that deviate significantly from cultural expectations. These patterns are pervasive and affect various aspects of a person’s life, including cognition, emotional regulation, interpersonal relationships, and impulse control.
Is OCD a Delusional Disorder?
No, OCD (Obsessive-Compulsive Disorder) is not classified as a delusional disorder. While there are some overlaps, they are fundamentally different. In OCD, individuals experience obsessions—intrusive thoughts or fears—and compulsions—repetitive behaviors performed in response to these obsessions. A key distinction is that people with OCD recognize their obsessions as irrational, whereas individuals with delusional disorder hold firm beliefs (delusions) and lack insight into their irrationality.
While those with OCD struggle with intrusive thoughts, they generally understand these thoughts do not reflect reality. They also recognize that their compulsions are excessive, yet still feel compelled to perform them to relieve anxiety. The research highlighted in a 2018 study published in Cambridge University Press titled “Obsessive-Compulsive Disorder and Delusions Revisited” shows that about 50% of individuals with OCD maintain a high level of insight, while around 15% exhibit “poor insight,” where their beliefs become more rigid and delusional-like but remain linked to OCD.
Is Body Dysmorphic Disorder Delusional?
Yes, Body Dysmorphic Disorder (BDD) is delusional. Both BDD and delusional disorders involve distorted beliefs. Individuals with BDD have strong convictions about perceived physical defects, while those with delusional disorder maintain fixed, false beliefs across various themes, not limited to appearance.
However, there are key differences between the two. A primary distinction is the degree of insight. Individuals with nondelusional BDD recognize that their beliefs about their appearance are inaccurate, whereas those with delusional disorder usually lack insight into the false nature of their beliefs. Additionally, BDD focuses specifically on perceptions of physical appearance, regarding flaws that are minimal or nonexistent. In contrast, delusional disorder encompasses a wider range of themes, including paranoia and grandiosity.
The diagnostic classification also differs significantly: BDD is categorized as an obsessive-compulsive and related disorder in the DSM-5, while delusional disorder is classified as a psychotic disorder. This distinction affects treatment approaches and our understanding of each condition’s underlying pathology. Notably, between one-third and 60% of individuals with BDD exhibit delusional features, according to a 2016 study by psychiatrist, Katharine A., published in CNS Spectrums titled “Delusional versus nondelusional body dysmorphic disorder: recommendations for DSM-5.” This highlights the complexity of BDD and the necessity for a nuanced diagnostic and treatment approach.
How Is Delirium Similar to Delusional Disorder?
Delirium is similar to delusional disorder because both conditions involve altered mental states and disturbances in cognition and perception. Individuals experience confusion, disorientation, and delusional beliefs in both cases, although the nature of these beliefs differs significantly.
In terms of onset, delirium presents rapidly, occurring within hours to days in response to acute medical issues such as infections or metabolic disturbances. It affects 20% of acute hospital patients and up to 62% of surgical patients, as indicated in a 2013 study published in the International Journal of Surgery titled “Delirium: A key challenge for perioperative care.” In contrast, delusional disorder has a more gradual onset, developing over weeks to months, and is usually linked to chronic psychological issues rather than acute medical conditions.
When examining symptoms, delirium includes confusion, impaired attention, fluctuating levels of consciousness, hallucinations, and disorganized thinking, with individuals potentially exhibiting agitation or lethargy. Delusional disorder, however, is characterized by persistent, non-bizarre delusions, with individuals lacking insight into the false nature of their beliefs. This condition does not involve the severe cognitive impairment seen in delirium.
Treatment approaches also vary. Delirium management focuses on identifying and addressing the underlying medical cause, which involves treating infections or correcting metabolic imbalances, along with supportive care to ensure a safe environment. Medications might be used to manage severe agitation or psychotic symptoms. Conversely, treatment for delusional disorder primarily involves psychotherapy, particularly cognitive-behavioral therapy, aimed at challenging and reframing delusional beliefs. Antipsychotic medications are prescribed, but the emphasis is on long-term management rather than acute intervention.
Which Conditions and Issues Are Commonly Related to Delusional Disorder?
The conditions that are commonly related to delusional disorders are mood disorders, anxiety disorders, substance use disorders, personality disorders, and psychotic disorders. These co-occurring conditions are explained below:

- Mood disorders: There is a significant overlap between delusional disorder and mood disorders, particularly depression and bipolar disorder. Individuals with these mood disorders develop delusions related to their emotional states.
- Anxiety disorders: Conditions such as generalized anxiety disorder and social anxiety disorder co-occur with delusional disorder. Anxiety exacerbates feelings of paranoia or irrational beliefs.
- Substance use disorders: Substance abuse, including alcohol and drug dependence, contributes to or worsens delusional symptoms. Withdrawal from substances also leads to the emergence of delusional thoughts.
- Personality disorders: Certain personality disorders, particularly paranoid personality disorder, are frequently seen alongside delusional disorder. The characteristics of paranoia in these disorders overlap with the delusions experienced.
- Psychotic disorders: While delusional disorder is classified separately, it occurs alongside other psychotic disorders, such as schizophrenia. Individuals experience similar symptoms, although the nature of their delusions and overall presentation differ.
These co-occurring conditions highlight the complexity of delusional disorder and the need for comprehensive assessment and treatment strategies that address both the delusions and any underlying or associated mental health issues.
Can Anxiety Disorders Cause Delusional Thinking?
Yes, anxiety disorders can cause delusional thinking. Anxiety significantly influences or exacerbates delusional thinking by heightening feelings of fear and worry. When individuals experience intense anxiety, their ability to think clearly and rationally becomes impaired. This heightened state of arousal leads to the development of irrational beliefs or delusions as a means of coping with overwhelming emotions.
For instance, in cases of social anxiety disorder, an individual develops delusional beliefs about being judged or persecuted by others. The constant fear of negative evaluation distorts their perception of reality, leading them to interpret benign interactions as threatening. Similarly, a generalized anxiety disorder causes individuals to catastrophize situations, leading to unfounded beliefs about danger or harm.
Moreover, anxiety triggers or amplifies paranoid thoughts, contributing to a sense of distrust and suspicion. When individuals are under significant stress, their cognitive resources are depleted, making it more challenging to critically evaluate their thoughts. As a result, they cling to delusions as a way to make sense of their anxiety, further entrenching these distorted beliefs.
Can Autistic People Develop Delusional Disorder?
Yes, autistic people develop delusional disorders. Individuals with autism spectrum disorders (ASD) are at an increased risk for delusional disorder. This occurs due to social and communicative challenges that make it difficult to interpret social cues, potentially leading to paranoid beliefs. Additionally, intense focus on specific interests evolves into fixed, delusional thoughts, especially if those interests involve themes of persecution, says a study by Michele. R., et al published in Frontiers in Psychiatry in 2022 titled “Recognizing Psychosis in Autism Spectrum Disorder.”
Heightened anxiety and stress, common in individuals with autism, also contribute to the development of delusional thinking as a coping mechanism. However, distinguishing between delusions and the idiosyncratic beliefs characteristic of ASD requires careful assessment by mental health professionals to ensure accurate diagnosis and treatment.
Can You Have Bipolar and Delusional Disorder Together?
Yes, you can have bipolar disorder and delusional disorder together. delusions are more common in individuals with bipolar disorder, particularly during manic episodes. The rates of delusions in bipolar disorder can range from 12% to 87%, depending on the phase of the disorder and the specific symptoms present, per a systematic review published in the World Journal of Psychiatry in 2022 titled “Psychotic symptoms in bipolar disorder and their impact on the illness.”
During manic episodes, for instance, individuals develop grandiose delusions, believing they possess special powers or abilities. In depressive phases, they might experience delusions of guilt or worthlessness. These overlapping symptoms complicate the clinical picture. Delusional disorder develops independently or as a result of the mood fluctuations characteristic of bipolar disorder.
Effective treatment requires careful differentiation between the two disorders, as the management strategies differ. Antipsychotic medications are necessary to address delusional symptoms, while mood stabilizers or antidepressants are used for bipolar disorder. A comprehensive treatment approach that addresses both conditions is essential for optimal outcomes.
Are Conspiracy Theorists Delusional?
Yes, conspiracy theorists exhibit delusional thinking, but this is not universally the case. From a psychological perspective, conspiracy theories stem from a desire to make sense of complex events or feelings of powerlessness. People find it reassuring to believe in a hidden agenda, as it provides a framework to explain their experiences or societal issues. This inclination does not necessarily indicate delusional disorder; rather, it reflects a cognitive bias where individuals interpret information selectively to confirm their beliefs, known as confirmation bias.
However, some conspiracy theories cross into delusional thinking, particularly when the beliefs are fixed and resistant to contrary evidence. In these cases, individuals firmly believe in conspiracies despite overwhelming evidence to the contrary, which aligns more closely with the characteristics of delusional disorder.
It’s important to note that not all conspiracy theorists have delusional disorders. Many individuals entertain conspiracy theories without developing a full-blown delusional belief system. The distinction lies in the degree of conviction and the impact on the individual’s life.